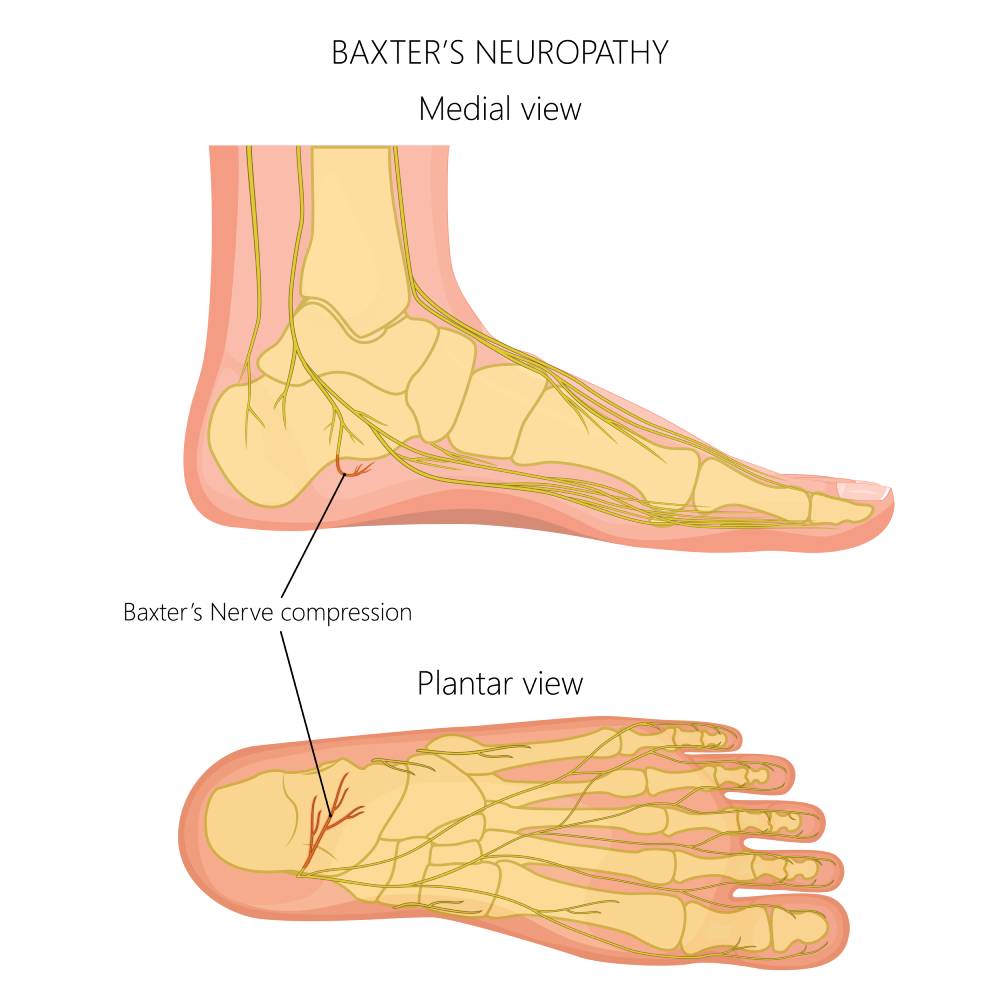
Also known as Baxter’s neuropathy, Baxter’s nerve entrapment is a condition in which one of the nerve’s travelling through the foot (the inferior calcaneal nerve) gets compressed between the surrounding structures, and subsequently inflamed, causing pain on the inner aspect of the heel. The nerve involved is the medial plantar nerve, which provides sensation to the skin of the arch of the foot and the inside of the heel.
It is a condition that develops over time, sometimes in the absence of any trauma or injury.
Baxter’s nerve entrapment can be caused by a variety of factors, such as wearing shoes that are too tight or poorly fitting, standing or walking for extended periods of time, and direct trauma to the foot.
Anatomy
The tibial nerve, which is a major nerve of the lower leg, is one of the two terminal branches of the sciatic nerve. When it enters the foot through the tarsal tunnel it splints into several branches.
Distal to this tunnel, the nerve gives off its terminal branches, the lateral and medial plantar nerves, which are responsible for sensory and motor functions of the foot.
Just after the splitting of these branches, the inferior calcaneal nerve arises, making it the first branch of the lateral plantar nerve.
Baxter’s nerve runs down between the abductor hallucis and the quadratus plantae muscles of the foot, and along the medial border of the long plantar ligament.
Being a mixed nerve, it also gives out sensory branches to the calcaneal periosteum, long plantar ligament, and the nearby vessels.
Symptoms of Baxter’s Neuropathy

Baxter’s nerve entrapment is estimated to be responsible for approximately 20 percent of chronic heel pain (Coles et al., 2021). It is a condition that is frequently overlooked, and the symptoms usually include:
-
- Pain in the heel or arch of the foot, which may be sharp or burning in nature.
-
- Tingling or numbness in the heel or arch of the foot.
-
- Swelling or tenderness around the affected area.
-
- Difficulty walking or standing for extended periods of time.
-
- Pain that worsens with activity, and improves with rest.
-
- A sensation of electric shock in the heel or arch of the foot.
Is my heel pain due to Baxter’s Neuropathy or Plantar Fasciitis?
Baxter’s nerve entrapment is often misdiagnosed as most of the cases of heel pain, especially in young adults, are attributed to plantar fasciitis (Prem & Anand, 2023).
Plantar fasciitis has symptoms similar to Baxter’s neuropathy and is the most common cause of heel pain, which is why clinicians may sometimes misdiagnose Baxter’s nerve entrapment as Plantar Fasciitis.
However, there are a few differentiating points. Pain directly beneath the heel is more common in Plantar Fasciitis
Also pain and stiffness that gets worse after periods of rest including after waking up in the morning, often occurs in plantar fasciitis.
In Baxter’s nerve entrapment, pain may be felt more on the medial arch of the foot and a sensation of numbness or pins and needles is also more likely as this involves compression of a nerve. It is always worth scanning the medial arch of the foot to ensure there isn’t a thickening or tendinosis of the medial component of the plantar fascia which may potentially have a secondary effect on the Baxter’s nerve.
In addition, palpation and scanning the abductor hallucis muscle on the medial arch of the foot is also important as this may swell or enlarge causing entrapment of the Baxter’s nerve.
Although Plantar fasciitis is distinct from Baxter’s neuropathy it can lead to the development of this condition.
What causes Baxter’s Nerve Entrapment?
There are quite a few reasons for the development of this condition. The nerve can get compressed between the inner muscles of the foot very easily due to its anatomical placement.
Common causes of Baxter’s neuropathy include:
-
- Poor posture leading to poor foot mechanics, including excess pronation.
-
- Having flat feet.
-
- Engaging in sports like running, which can cause compression due to overuse.
-
- Atrophy of the heel pad muscles.
-
- Development of bony spurs on the calcaneus impinging the nerve.
-
- Entrapment due to wearing poorly fitting shoes.
-
- Trauma or injury to the heel which causes swelling.
-
- Obesity.
-
- Plantar fasciitis.
-
- Hypertrophy of the Abductor Hallucis muscle of the foot.
Diagnosis
A careful medical history and a detailed physical exam pave way for a correct diagnosis (Along with that, a few diagnostic tests may be necessary, including:
-
- Xray – to rule out spurs, fractures, or other bony deformities.
-
- MRI – great for imaging the soft tissues, it can show signs of compression in the inferior calcaneal nerve including atrophy of abductor digiti quinti muscle, plantar fasciitis (if present), and edema around the calcaneum (Chundru et al., 2008).
-
- Ultrasound: usually to exclude Plantar Fasciitis as the cause of the pain.
-
- Ultrasound guided nerve block – a local anesthetic agent such as lidocaine, is injected at the origin of Baxter’s nerve under the guidance of an ultrasound. If the pain stops, it is diagnostic for this condition.
Treatment and Management
Baxter’s nerve entrapment causes a lot of discomfort, and the pain is usually managed by rest, icing, and giving over the counter NSAIDs like ibuprofen or naproxen. Patients are advised to take a break from strenuous physical activity, and in cases of severe pain stronger analgesics are prescribed. Steroid injections or nerve hydro dissection can help minimize the inflammation around the nerve, reducing pain and promoting healing.
Soft tissue massage and mobilization techniques can help alleviate the pressure on the nerve. Orthotics (inner soles for the shoes) can be utilized. Physical therapy is an important part of the management of this condition, and certain stretching exercises can be incorporated to help with the recovery process.
Injections for Baxter’s nerve entrapment
Nerve hydro dissection is an effective treatment for Baxter’s nerve entrapments, in which an anesthetic, saline, or 5% dextrose solution is used to separate the nerve from its surrounding tissues, like fascia, muscles, or ligaments, under the guidance of an ultrasound (Lam et al., 2020). In the case of Baxter’s neuropathy, the inferior calcaneal nerve is blocked in this manner, and this technique provides rapid, effective, and long-lasting resolution of pain.
Ultrasound guided radiofrequency ablation is a procedure that involves using sound waves to heat the Baxter’s nerve to 90 degrees, causing a semi-permanent numbing of the nerve.
It prevents the nerve from transmitting pain signals, and leads to the formation of new blood vessels, thereby accelerating healing. The ablation needle is guided by ultrasound, and after administering a local anesthetic.
In a few cases, surgery may be performed to decompress the nerve. However, that is generally done as a last resort in cases which have failed to respond to other treatments.
Conclusion
Baxter’s nerve entrapment can become a chronic condition if timely intervention is not done. However, following an accurate treatment plan can not only manage pain, but help improve the overall quality of life and allow the patient to resume physical activity
References
Chundru, U. et al. (2008) Plantar fasciitis and calcaneal spur formation are associated with abductor digiti minimi atrophy on MRI of the foot – skeletal radiology, SpringerLink. Journal of the International Skeletal Society A Journal of Radiology, Pathology and Orthopedics.
Coles, I.R. et al. (2021) Ultrasound block of first branch of the lateral plantar nerve (Baxter nerve): Case report of a promising and effective treatment for heel chronic pain, Science Direct. Brazilian Journal of Anesthesiology (English Edition).
Kim, B.S. et al. (2015) Branching patterns of medial and inferior calcaneal nerves around the tarsal tunnel, Annals of Rehabilitation Medicine. Korean Academy of Rehabilitation Medicine.
Lam, K.H.S. et al. (2020) Ultrasound-guided nerve hydrodissection for pain management: Rationale, methods, current literature, and Theoretical Mechanisms, Journal of pain research. U.S. National Library of Medicine
Prem, A. and Anand, S. (2023) Baxter’s nerve injury: an often-overlooked cause of chronic heel pain: a case report, HSPI. Archives of Clinical and Experimental Orthopedics.